
Adrenal Gland Surgery (Adrenalectomy)
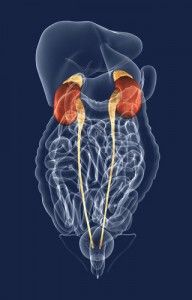 The adrenal gland is a member of the endocrine gland family. These small, paired triangular shaped glands reside above each kidney. Though small in size, the adrenal glands control a myriad of important bodily functions. These include blood pressure control, bodily hormone production and management, water regulation by the kidneys, blood sugar usage, and the “fight or flight” reaction during times of stress. Adrenal-produced hormones include cortisol, aldosterone, and adrenaline (i.e., epinephrine and norepinephrine). A small portion of the body’s male and female sex hormones (i.e., estrogen and androgens) are included as well.
The adrenal gland is a member of the endocrine gland family. These small, paired triangular shaped glands reside above each kidney. Though small in size, the adrenal glands control a myriad of important bodily functions. These include blood pressure control, bodily hormone production and management, water regulation by the kidneys, blood sugar usage, and the “fight or flight” reaction during times of stress. Adrenal-produced hormones include cortisol, aldosterone, and adrenaline (i.e., epinephrine and norepinephrine). A small portion of the body’s male and female sex hormones (i.e., estrogen and androgens) are included as well.
Surgical adrenal gland disease is generally related to a growth on one of the glands. The far majority of adrenal gland diseases are benign (i.e., not cancerous). Approximately 80% of adrenal tumors are identified during an abdominal X-ray being performed for an unrelated reason. These are called “incidentalomas.” Some of these tumors will be found to produce an excess of hormones. Others will have no identifiable function at all. Malignant (i.e., cancerous) adrenal tumors do occur. These comprise approximately 10-15% of “incidentalomas.”
The surgical management of adrenal disease, whether benign or malignant, involves removing the abnormal gland. This is most often performed through a minimally invasive laparoscopic approach unless technically not feasible.
Symptoms of Adrenal Gland Problems
Patients with adrenal gland abnormalities may present with no symptoms (“incidentaloma”). Others present as a result of the over-production of a specific hormone. Adrenal tumors associated with excess hormone production include pheochromocytomas, aldosterone secreting tumors, and cortisol secreting tumors:
- Pheochromocytomas produce excess adrenaline-type hormones. These classically present with the triad of a headache, sweating, and palpitations. Sometimes, patients may present with uncontrollable blood pressure, anxiety, blurred vision, nausea or vomiting, and/or a rapid heart rate. Symptoms may last from a few seconds to several minutes. These tumors can be benign or malignant. The larger the size, the greater the malignant potential. Some of these tumors run in families while others are sporadic (i.e., have no predisposing reason for growing).
- Aldosterone-producing tumors cause high blood pressure and low blood potassium levels. These can be present in up to 10-15% of patients with hypertension. In some patients, this may result in symptoms of weakness, fatigue, and frequent urination. This is called Conn Syndrome. Surgical management of an adrenal tumor proven to produce excess aldosterone is generally curative.
- Cortisol-producing tumors refer to patients who have Cushing Syndrome. Such manifestations include obesity (especially of the face and trunk), high blood sugar, high blood pressure, menstrual irregularities, fragile skin and prominent stretch marks (striae). Some patients present with anxiety and a “steroid induced psychosis” from the excess hormones. Other causes of cortisol overproduction may include tumors of the pituitary gland, thymus gland, lung or pancreas. Over-ingestion of steroid hormones can also cause some of the above symptoms. Surgical management of an adrenal tumor proven to produce excess cortisol is generally curative.
- An incidentally found mass refers to any adrenal mass found incidentally during an abdominal X-ray for an unrelated reason. By definition, an incidentaloma is usually at least 1cm or larger in size. Some of these tumors are functioning. This means that they are producing excess some type of excess hormone as described in the preceding sections. Others do not produce any hormones at all. Most incidentally found adrenal masses do not produce excess hormones, cause no symptoms, and are benign. Surgical removal of incidentally discovered adrenal tumors is indicated if:
- The tumor is found to produce excess hormones
- Is large in size (more than 4-6 centimeters)
- If there is a suspicion that the tumor could be malignant.
- Adrenal gland cancers (adrenal cortical cancer) are rare tumors that are usually very large at the time of diagnosis. Removal of these tumors may be preferentially done by open adrenal surgery instead of a minimally invasive laparoscopic approach.
Evaluation of Adrenal Gland Disease
If an adrenal tumor is suspected based on symptoms or has been identified by X-ray, the patient should undergo blood and urine tests to determine if the tumor is over-producing hormones. Special X-ray tests, such as a CT scan, nuclear medicine scan, MRI or selective venous sampling are commonly used to locate the suspected adrenal tumor. Biopsy of an adrenal gland is rarely indicated prior to surgery. The only times this may be recommended is if there is suspicion of a metastatic tumor from a melanoma, lymphoma, lung, kidney, breast or intestinal cancer.
Surgical removal of the adrenal gland is the preferred treatment for patients with adrenal tumors that secrete excess hormones and for primary adrenal tumors that appear malignant.
Adrenalectomy
Laparoscopic (minimally invasive) surgery is the preferred approach for most adrenalectomies. Unlike open surgery which requires a larger incision, laparoscopic adrenal gland surgery requires only three or four 1/4 to 1/2 inch incisions. A tiny camera is inserted which allows excellent visualization of the abnormal gland. With the use of small dissecting instruments, the gland is removed intact.
Occasionally, open surgery is required to remove the adrenal glands. This approach is chosen if the gland appears cancerous or is very large in size. This option is discussed prior to surgery. Sometimes difficulty arises during laparoscopic surgery and the operation is converted to a traditional (or open) approach.
Adrenal gland surgery is conducted as follows:
- The surgery is performed under a complete general anesthesia so that the patient is asleep during the procedure and feels no pain.
- For laparoscopic surgery, a laparoscope is connected to a special TV camera. This gives the surgeon a magnified view of the adrenal gland.
- It is almost always necessary to remove the entire adrenal gland in order to safely remove the tumor.
- After the surgeon removes the adrenal gland, the small incisions are closed.
Getting Back to Normal
- Post-operative pain is generally mild and can be regulated with a prescription narcotic.
- Patients are able to shower the day after surgery and engage in light activity.
- Patients are allowed to return to their normal activities about a week after surgery with a laparoscopic approach. Open surgery requires approximately one month for the incision to heal.
- Patients with cortisol-producing tumors and Cushing’s Syndrome will need to remain on tapering doses of prednisone (cortisol pills) after surgery. Blood tests are used periodically to assess the remaining adrenal glands recovery after surgery. An Endocrinologist is frequently involved in managing your postoperative steroid needs.
- Patients with an aldosterone-producing tumor will need to have their serum potassium level checked after surgery and may need to continue to take medications to control their blood pressure.
Please be sure to schedule a post-op appointment 7-14 days after your surgery, so the doctor can evaluate your recovery progress.